A 72-year-old man presents to the emergency department after briefly losing consciousness while walking to his mailbox. He regained consciousness within 30 seconds. He denies preceding chest pain, palpitations, nausea, or diaphoresis. During the past month, he has had several episodes of unexplained lightheadedness. His medical history includes hypertension, type 2 diabetes mellitus, and an anterior myocardial infarction 4 years ago. Medications include aspirin, atorvastatin, lisinopril, metformin, and metoprolol succinate. He has taken no additional doses and denies using digoxin or nonprescription medications. Temperature is 36.7°C (98.1°F), blood pressure is 132/74 mm Hg, pulse is 42/min, and respiratory rate is 14/min. Oxygen saturation is 98% on room air. He is alert and appears comfortable. Cardiac examination reveals a slow, regular rhythm without murmurs. The lungs are clear, and there is no peripheral edema. Laboratory studies, including serum potassium, magnesium, calcium, and thyroid-stimulating hormone, are normal. Serial high-sensitivity troponin levels are negative.
 Which of the following is the most appropriate next step in management?
Which of the following is the most appropriate next step in management?
The correct answer is:
B) Implant a permanent pacemaker
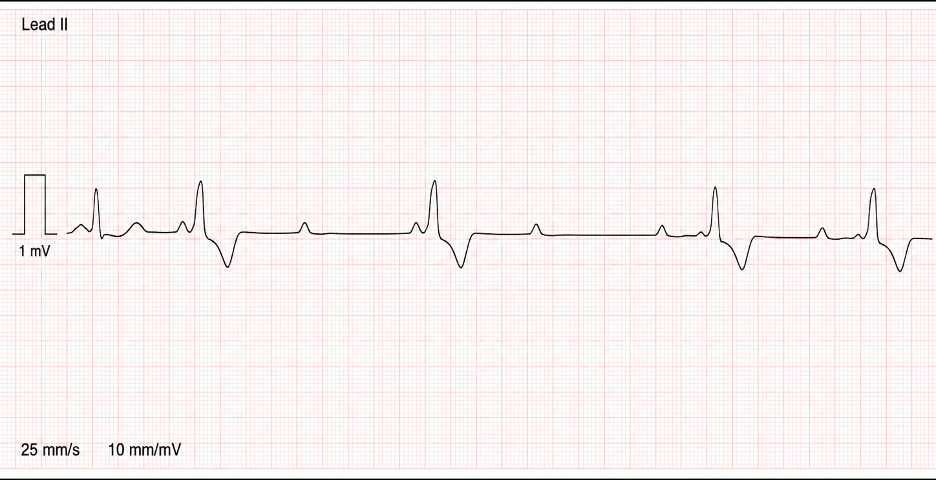
This patient has symptomatic second-degree atrioventricular block, Mobitz type II. The diagnosis is supported by intermittent nonconducted P waves without progressive prolongation of the PR interval. The wide QRS complex and concomitant bundle branch block suggest that the conduction defect is located below the AV node within the His-Purkinje system.
Mobitz II block is clinically important because the diseased infranodal conduction system can fail abruptly, causing progression to complete heart block, severe bradycardia, syncope, or sudden cardiac death. His unexplained syncope and recurrent presyncope indicate that the conduction abnormality is already producing clinically significant cerebral hypoperfusion. Permanent pacemaker implantation is therefore indicated.
Potentially reversible causes of bradycardia should always be assessed. Beta blockers can slow AV nodal conduction, but medication effect alone is less likely to produce an infranodal Mobitz II pattern with a wide QRS complex and fixed PR intervals. Although metoprolol should be held during evaluation, medication withdrawal does not eliminate the need for pacing in a patient with symptomatic Mobitz II block and structural conduction disease.
A useful distinction is that Mobitz type I block usually occurs within the AV node and demonstrates progressive PR prolongation before a dropped QRS complex. It is often transient and benign. Mobitz type II block occurs below the AV node, has constant PR intervals before dropped beats, and requires pacing because of its unpredictable progression.
Answer choice A: Discontinue metoprolol and arrange outpatient rhythm monitoring, is incorrect.
Holding AV nodal–blocking medications is appropriate during the initial evaluation of bradycardia. However, outpatient observation alone is unsafe in a patient with syncope and an ECG demonstrating infranodal Mobitz II block. The wide QRS complex and bundle branch block indicate advanced His-Purkinje disease that may progress suddenly to complete heart block even after metoprolol is discontinued.
Answer choice C: Initiate intravenous atropine as definitive therapy, is incorrect.
Atropine increases sinus rate and AV nodal conduction by blocking parasympathetic activity. It may temporarily improve symptomatic bradycardia caused by AV nodal disease, particularly Mobitz type I block. However, Mobitz II block is usually infranodal and often responds poorly to atropine. Atropine can serve as a temporary measure in selected unstable patients, but it does not provide definitive protection against complete heart block.
Answer choice D: Perform radiofrequency ablation of the atrioventricular node, is incorrect.
AV nodal ablation intentionally creates complete heart block and is sometimes used with permanent pacing for refractory atrial fibrillation with uncontrolled ventricular rates. This patient already has pathologic conduction failure and no tachyarrhythmia requiring ablation. Destroying additional conduction tissue would worsen the underlying problem.
Answer choice E: Reassure the patient and repeat the ECG in 6 months, is incorrect.
Observation may be reasonable for asymptomatic first-degree AV block or selected cases of Mobitz type I block. Symptomatic Mobitz II block carries a substantial risk of progression to complete heart block and requires prompt permanent pacing rather than surveillance.
Key Learning Point
Mobitz type II AV block is characterized by fixed PR intervals with intermittent nonconducted P waves and often reflects infranodal His-Purkinje disease. Because it can abruptly progress to complete heart block, symptomatic patients require permanent pacemaker implantation.
