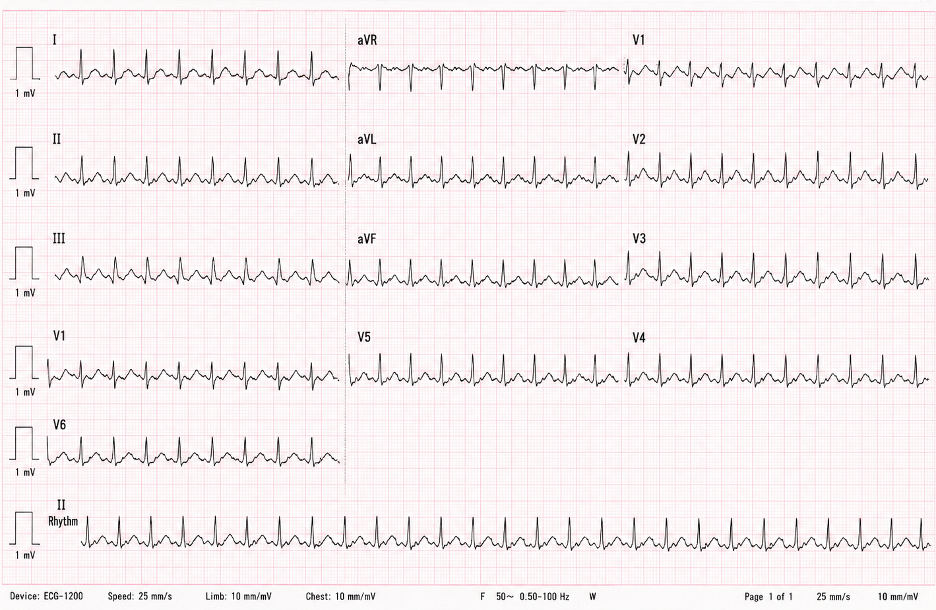
A 66-year-old woman presents to the emergency department because of palpitations and mild shortness of breath that began earlier that morning. She denies chest pain, syncope, or focal neurologic symptoms. Her medical history includes hypertension, severe persistent asthma, and hyperlipidemia. She has no known history of coronary artery disease or heart failure. Medications include losartan, atorvastatin, an inhaled corticosteroid, and albuterol. Temperature is 36.8°C (98.2°F), blood pressure is 126/78 mm Hg, pulse is 148/min and regular, respiratory rate is 18/min, and oxygen saturation is 97% on room air. On physical examination, she appears mildly anxious but is alert and speaking in complete sentences. Jugular venous pressure is normal, the lungs are clear, and there is no peripheral edema. ECG demonstrates a regular narrow-complex tachycardia at 150/min (see image below) Transthoracic echocardiography performed 3 months ago showed normal ventricular systolic function and no significant valvular disease.
Which of the following is the most appropriate initial treatment?
The correct answer is:
C) Diltiazem
This patient has atrial flutter with 2:1 atrioventricular conduction, producing the characteristic ventricular rate of approximately 150/min. The continuous sawtooth atrial activity in the inferior leads is also typical. She is symptomatic but hemodynamically stable, with preserved blood pressure, normal mental status, no ischemic chest discomfort, and no evidence of acute heart failure. The appropriate initial treatment is therefore ventricular rate control.
Diltiazem slows conduction through the atrioventricular node and reduces the ventricular response without directly terminating the atrial flutter circuit. It is particularly appropriate in this patient because she has preserved left ventricular systolic function and severe asthma, which makes beta-blocker therapy less desirable due to the risk of bronchospasm.
Atrial flutter is caused by a macroreentrant atrial circuit, most commonly involving the right atrium. The atrial rate is typically close to 300/min, and 2:1 conduction through the AV node produces a ventricular rate near 150/min. Rate control can be achieved with a non-dihydropyridine calcium channel blocker or a beta blocker. Anticoagulation decisions follow the same thromboembolic risk framework used for atrial fibrillation. Definitive treatment for recurrent typical atrial flutter is catheter ablation of the cavotricuspid isthmus, which has a high success rate.
Answer choice A: Adenosine, is incorrect.
Adenosine transiently blocks conduction through the AV node and can expose underlying flutter waves when the diagnosis is uncertain. However, it generally does not terminate atrial flutter because the reentrant circuit is located within the atrium and does not depend on the AV node. In this patient, the flutter waves are already visible, so adenosine would provide little therapeutic benefit.
Answer choice B: Amiodarone, is incorrect.
Amiodarone can be used for rhythm control in selected atrial arrhythmias, particularly when structural heart disease limits other options. However, it is not the preferred initial therapy for a stable patient whose immediate need is ventricular rate control. Its slow onset and substantial long-term toxicities, including pulmonary, hepatic, thyroid, ocular, and dermatologic adverse effects, make it less appropriate than diltiazem in this setting.
Answer choice D: Electrical cardioversion, is incorrect.
Synchronized cardioversion is the treatment of choice when atrial flutter causes hemodynamic instability, such as hypotension, altered mental status, ongoing ischemia, or acute pulmonary edema. It may also be used electively for rhythm restoration after appropriate evaluation of thromboembolic risk. This patient is stable, so pharmacologic rate control is the appropriate first step.
Answer choice E: Flecainide, is incorrect.
Flecainide is a class IC antiarrhythmic drug that may be used for rhythm control in carefully selected patients without structural heart disease. It is not used as the initial treatment of atrial flutter with rapid ventricular response because it does not provide reliable AV nodal rate control. In addition, class IC agents can slow the atrial flutter rate enough to permit dangerous 1:1 AV conduction unless they are combined with an AV nodal–blocking medication.
Key Learning Point
Atrial flutter with 2:1 AV conduction commonly produces a regular ventricular rate near 150/min. Hemodynamically stable patients should initially receive AV nodal rate control, whereas unstable patients require synchronized cardioversion.
