A 57-year-old woman is hospitalized for community-acquired pneumonia. Her medical history includes hypertension, major depressive disorder, and chronic kidney disease. Her home medications are hydrochlorothiazide, escitalopram, and lisinopril. On admission, she is started on intravenous azithromycin and ceftriaxone. On hospital day 2, she reports palpitations and suddenly loses consciousness. Temperature is 37.4°C (99.3°F), blood pressure is 104/66 mm Hg, pulse is 96/min, respiratory rate is 18/min, and oxygen saturation is 96% on room air. Telemetry is shown (see image below).
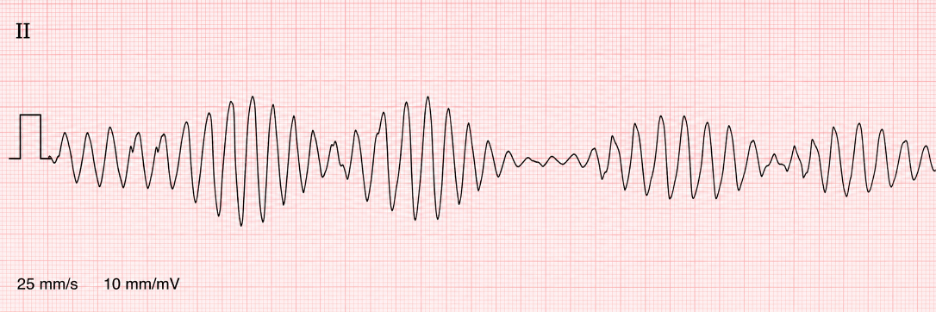 The rhythm terminates spontaneously after approximately 20 seconds, and she regains consciousness. She is alert but anxious. Cardiac and pulmonary examinations are otherwise unchanged.
The rhythm terminates spontaneously after approximately 20 seconds, and she regains consciousness. She is alert but anxious. Cardiac and pulmonary examinations are otherwise unchanged.
Laboratory studies show:
Potassium: 2.9 mEq/L
Magnesium: 1.4 mg/dL
Creatinine: 1.9 mg/dL
Troponin I: normal
A 12-lead ECG obtained after the episode demonstrates sinus rhythm with a corrected QT interval of 560 milliseconds.
Which of the following is the most appropriate immediate treatment?
The correct answer is:
C) Intravenous magnesium sulfate
This patient has torsades de pointes, a form of polymorphic ventricular tachycardia associated with prolonged ventricular repolarization. The diagnosis is supported by transient syncope, a polymorphic wide-complex rhythm that twists around the baseline, and marked QT prolongation after the episode.
Multiple risk factors have combined to prolong the QT interval in this patient. Escitalopram and azithromycin can both delay ventricular repolarization, while hydrochlorothiazide has contributed to hypokalemia and hypomagnesemia. Chronic kidney disease may further increase medication exposure and electrolyte instability. These factors promote early afterdepolarizations, which can trigger torsades de pointes.
Intravenous magnesium sulfate is the first-line treatment, even when the serum magnesium level is normal. Magnesium suppresses early afterdepolarizations and stabilizes myocardial electrical activity. The offending QT-prolonging medications should be discontinued, and potassium and magnesium deficits should be corrected aggressively. If recurrent episodes occur in the setting of bradycardia, temporary overdrive pacing or isoproterenol may be required to shorten the QT interval.
Because this episode terminated spontaneously and the patient is currently stable, immediate electrical shock is not required. However, sustained torsades causing hemodynamic instability or loss of a pulse requires immediate unsynchronized defibrillation.
Answer choice A: Intravenous amiodarone, is incorrect.
Amiodarone is commonly used for monomorphic ventricular tachycardia and several atrial arrhythmias. However, it can prolong the QT interval and may worsen torsades de pointes. Although amiodarone has a relatively low torsades risk compared with some other class III drugs, it should not be used to treat a ventricular arrhythmia driven by marked QT prolongation.
Answer choice B: Intravenous lidocaine, is incorrect.
Lidocaine may be used for selected ventricular arrhythmias, particularly those associated with acute myocardial ischemia. It does not address the early afterdepolarizations caused by acquired QT prolongation and is not first-line therapy for torsades de pointes. Magnesium administration and removal of the precipitating factors are more appropriate.
Answer choice D: Oral metoprolol, is incorrect.
Beta blockers are important in congenital long-QT syndromes because they reduce adrenergically triggered arrhythmias. However, this patient has acquired QT prolongation caused by medications and electrolyte depletion. Oral metoprolol would not provide sufficiently rapid treatment and could worsen bradycardia, potentially increasing the risk of recurrent torsades in pause-dependent acquired long-QT syndrome.
Answer choice E: Synchronized electrical cardioversion, is incorrect.
Synchronized cardioversion is used for unstable tachyarrhythmias with an organized QRS complex. Torsades de pointes is polymorphic, making reliable synchronization difficult. If the arrhythmia is sustained and causes instability, immediate unsynchronized defibrillation is indicated. This patient’s rhythm has already terminated, so intravenous magnesium is the appropriate immediate therapy to prevent recurrence.
Key Learning Point
Torsades de pointes is a polymorphic ventricular tachycardia associated with QT prolongation. Immediate treatment is intravenous magnesium sulfate, correction of potassium and magnesium abnormalities, and discontinuation of QT-prolonging medications; unstable sustained episodes require unsynchronized defibrillation.
