A 28-year-old man presents to the emergency department because of sudden-onset palpitations, lightheadedness, and mild shortness of breath that began 45 minutes ago. He has experienced several prior episodes of rapid heartbeat that terminated spontaneously, but the current episode feels faster and more irregular. He denies chest pain or syncope. His medical history is otherwise unremarkable, and he takes no medications. His father died suddenly at age 42, although the cause was never established. Temperature is 36.8°C (98.2°F), blood pressure is 112/70 mm Hg, pulse is rapid and irregular, respiratory rate is 18/min, and oxygen saturation is 98% on room air. On physical examination, h is alert and speaking comfortably. The lungs are clear, and the extremities are warm with normal capillary refill.
 Review of an ECG obtained during a prior asymptomatic visit shows a short PR interval, a slurred initial upstroke of the QRS complex, and a widened QRS complex.
Review of an ECG obtained during a prior asymptomatic visit shows a short PR interval, a slurred initial upstroke of the QRS complex, and a widened QRS complex.
Which of the following is the most appropriate initial treatment?
The correct answer is:
C) Intravenous procainamide
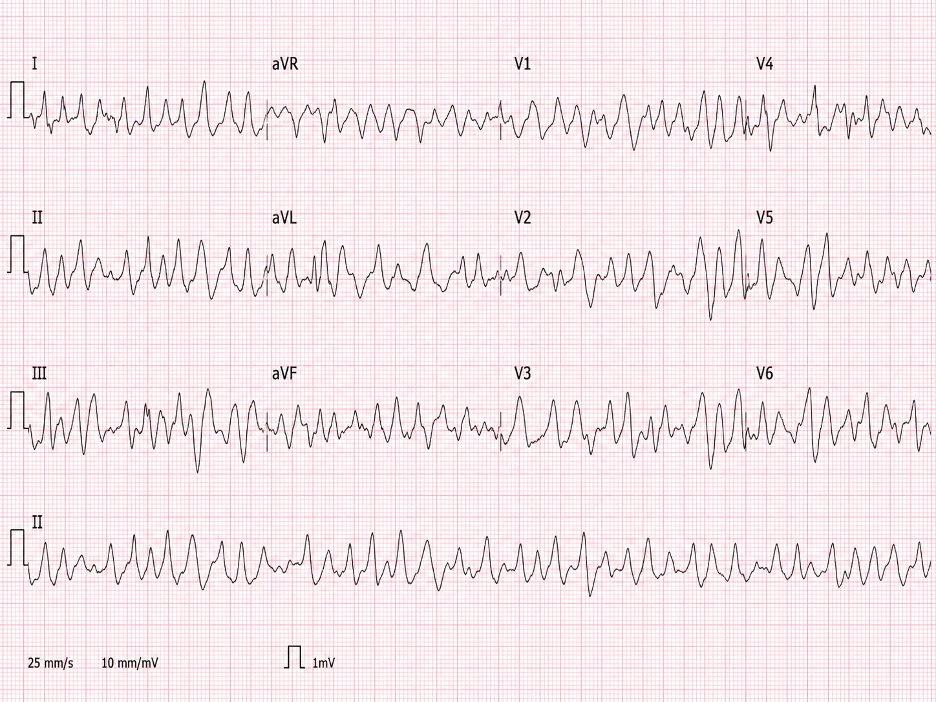
This patient has atrial fibrillation with ventricular preexcitation due to Wolff-Parkinson-White syndrome. The prior ECG findings of a short PR interval, delta wave, and widened QRS complex indicate the presence of an accessory atrioventricular pathway. During atrial fibrillation, rapid atrial impulses can travel through this pathway directly to the ventricles, bypassing the normal rate-limiting function of the AV node.
The resulting ECG is an irregularly irregular wide-complex tachycardia with extremely rapid ventricular rates and beat-to-beat variation in QRS morphology. The variable QRS appearance reflects differing degrees of ventricular activation through the accessory pathway and the normal His-Purkinje system. This rhythm is dangerous because extremely rapid ventricular activation can degenerate into ventricular fibrillation.
Because the patient is currently hemodynamically stable, intravenous procainamide is appropriate. Procainamide slows conduction through the accessory pathway and can terminate the arrhythmia. Ibutilide is another potential option in a stable patient. If hypotension, altered mental status, ischemic chest discomfort, pulmonary edema, or other evidence of instability develops, immediate synchronized cardioversion is required.
AV nodal–blocking medications are contraindicated in preexcited atrial fibrillation. Blocking the AV node can preferentially direct atrial impulses through the accessory pathway, increasing the ventricular rate and potentially precipitating ventricular fibrillation. This principle applies even to medications that are routinely used for atrial fibrillation without preexcitation.
Answer choice A: Intravenous adenosine, is incorrect.
Adenosine transiently blocks AV nodal conduction and is effective for AV node–dependent reentrant tachycardias, including many cases of orthodromic atrioventricular reentrant tachycardia. However, this patient has atrial fibrillation with ventricular preexcitation rather than a regular AV node–dependent tachycardia. AV nodal blockade may increase conduction through the accessory pathway and trigger ventricular fibrillation.
Answer choice B: Intravenous diltiazem, is incorrect.
Diltiazem is commonly used for ventricular rate control in ordinary atrial fibrillation. In preexcited atrial fibrillation, however, slowing AV nodal conduction allows more atrial impulses to reach the ventricles through the accessory pathway. This can accelerate the ventricular response and cause hemodynamic collapse or ventricular fibrillation.
Answer choice D: Intravenous propranolol, is incorrect.
Beta blockers reduce AV nodal conduction and are appropriate for rate control in many supraventricular arrhythmias. They should be avoided in atrial fibrillation with Wolff-Parkinson-White syndrome because they do not block the accessory pathway and may promote dangerously rapid preexcited ventricular conduction.
Answer choice E: Intravenous verapamil, is incorrect.
Verapamil is another AV nodal–blocking medication that may be used for selected supraventricular tachyarrhythmias. In this patient, it could suppress the normal AV nodal route while leaving the accessory pathway unopposed, increasing the risk of ventricular fibrillation. It is therefore contraindicated.
Key Learning Point
Atrial fibrillation with Wolff-Parkinson-White syndrome produces an irregular, very rapid, wide-complex rhythm with variable QRS morphology. Stable patients should receive procainamide or ibutilide. AV nodal–blocking medications are contraindicated because they may accelerate accessory-pathway conduction and precipitate ventricular fibrillation.
